
Alive Blog
“Pinched nerve” (or “trapped nerve”)
Popular myth or real problem?
“Pinched nerve” is one of those expression that – as chiropractors – we hear often in practice. In fact, paired with “sciatica“, “lower back pain”, or simply “pain”, it is one of the most common. Can a nerve be “pinched”, “trapped”, “impinged”? What happens on a physical level when we use these expressions? Aim of this post is to bring some data and the latest research on what a “pinched” nerve really is, how it presents and what to do in order to get relief.
What
First of all, what is a “pinched nerve”? You might not believe me, but there are over 7 trillion (that’s a “7” with 12 “zeros”, 7.000.000.000.000) in the human body. They come in all sorts of lenghts, size, diameter, shape, function. Think about the nerves in your body as the electrical wiring system that connects your brain (the elaboration centre), the spinal cord and the rest of the body. Nerves innervate EVERYTHING in your body. Muscles, glands, organs, tissues, blood vessels, other nerves, literally everything is controlled by nerves. For obvious reasons, it would be impossible to classify all of them; however I can provide a list of the major nerves in the body.
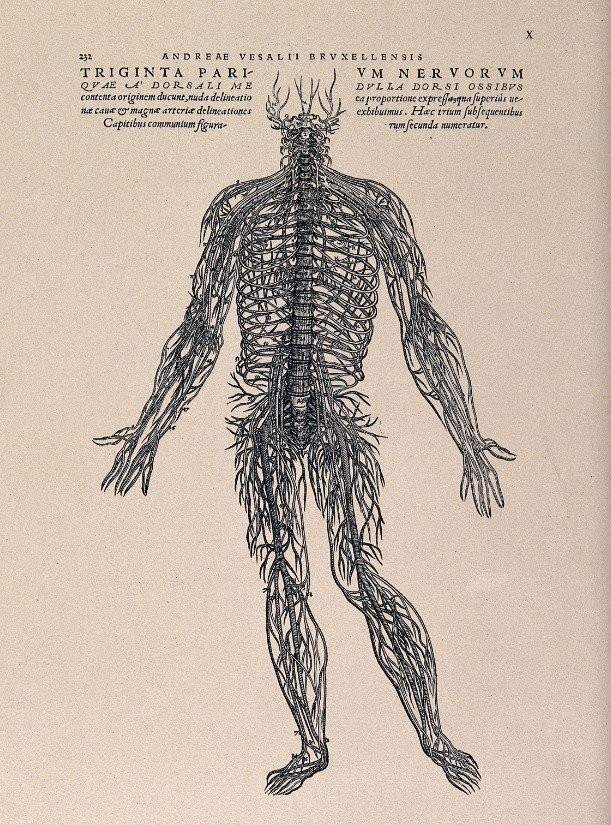
Think about the brain and spinal cord as the main strcutres from which every single nerve develops. All the nerves in the body are either a continuation of the 31 pairs of SPINAL NERVES (that come out from the little holes on the side of each vertebra, which we also discuss HERE); or the come out directly from the skull (just above the neck, and these are called CRANIAL NERVES).
Spinal nerves
Cervical Nerves (C1-C8):
- They control the arms in terms of sensation and muscle action.
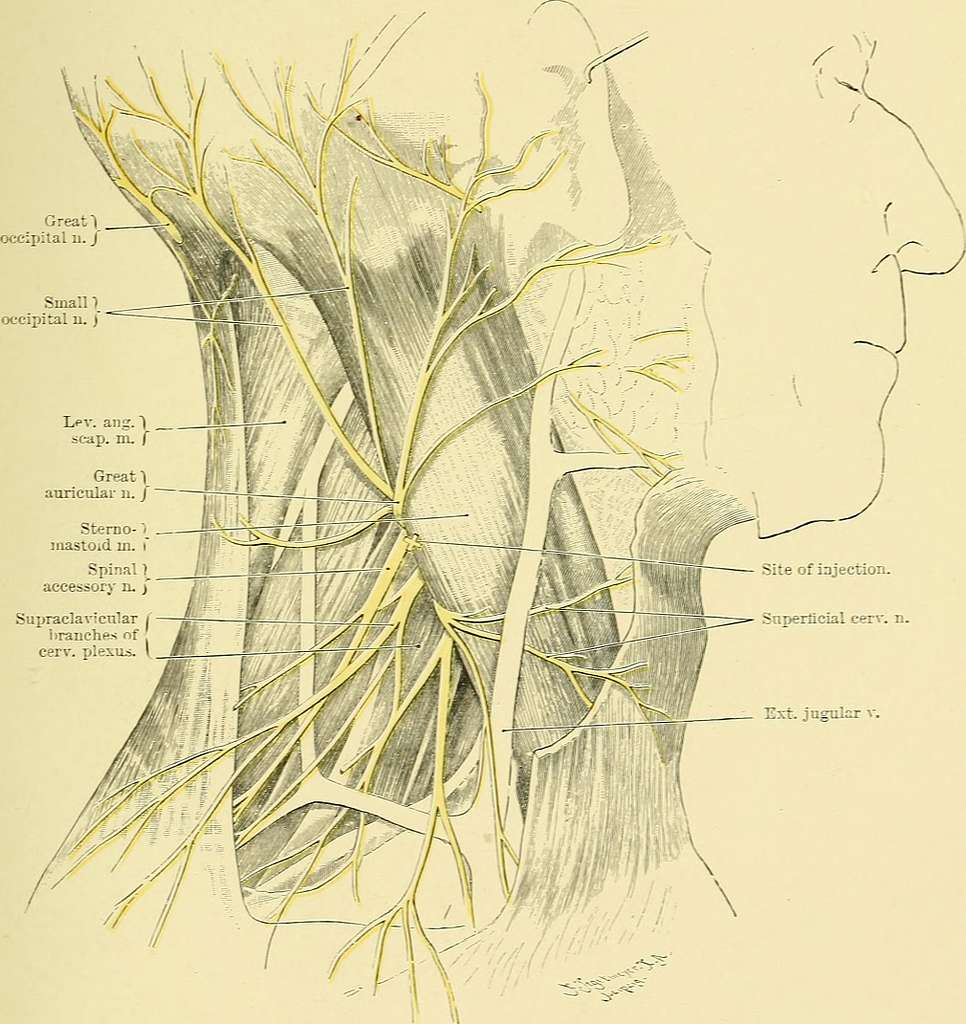
- Cervical plexus: muscle control of upper torso and neck + sensation in occiput (back of the head), shoulders and neck
- Phrenic nerves: muscle control of the respiration process (diaphragm, pecs, traps, sternocleidmastoid, intercostals).
Thoracic Nerves (T1-T12):
- They innervate various organs in the body (lungs, heart, liver, stomach, small intestine)
- Intercostal nerves: sensory information from the chest and abdomen + motor function of intercostal muscles and abdominal wall
- Subcostal nerves: subcostal means (under the ribs) and this nerves supply various muscles in the abdomen
Lumbar Nerves (L1-L5):
- They innervate everything below the belt line in terms of function, sensation and muscle action.
- Femoral nerve: motor and sensory information to various areas of the legs
- Obturator nerve: motor + sensory info to and from the inner tigh
- Sciatic nerve: motor and sensory (back of the leg). Largest nerve in the human body (and one of those who gets “trapped” quite easily). Duyring my years in practice, I can say between 50 to 70% of my clients had sciatic pain in their life.
Sacral Nerves (S1-S5):
- Sciatic Nerve: forms from branches originating from the lumbars and from the sacrum. It is composed of two major branches: Tibial Nerve and Common Peroneal Nerve
- Pudendal Nerve: movement and sensation in the pubic region / genital area / genitals function
Coccygeal Nerve (Co1):
- Coccygeal Plexus: supplies the sacrotuberal ligament as well as skin over the coccyx
These nerves are part of the peripheral nervous system and play a crucial role in transmitting signals between various parts of the body and the central nervous system (brain and spinal cord). They control sensations, motor functions, and autonomic functions of different regions. Keep in mind that there are many other smaller branches and variations of these nerves, but the ones listed above are some of the major ones derived from spinal nerves.
Cranial nerves
These are a special type of nerves because they are the only one to emerge directly from the brain, rather than from the spinal cord. During my 5 year course at the AECC in Bournemouth, studying these nerves became basically an obsession, especially because the functions they carry out are very complex and intricate (some of them control tiny muscles in the eye, some of them control salivary glands and face muscles, etc). Differently from the spine, where the exit points are all the same (the so called intervertebral foramen), the cranial nerves come out from different holes in the skull and identifying each of them is not easy. This is why we carried out so many dissection classes with real human specimens as well. I will never forget those lectures in the “wet lab”, and I feel very lucky for the chance the AECC gave us as students back in the days.
There are 12 pairs of cranial nerves, and they are usually identified with roman numbers)
Olfactory Nerve (CN I):
- Function: Sensory
- Function: Olfaction (sense of smell)
Optic Nerve (CN II):
- Function: Sensory
- Function: Vision
Oculomotor Nerve (CN III):
- Function: Motor
- Function: Controls most eye movements, including constriction of the pupil and adjusting the lens for focusing.
Trochlear Nerve (CN IV):
- Function: Motor
- Function: Controls movement of the superior oblique muscle of the eye.
Trigeminal Nerve (CN V):
- Function: Mixed (Sensory and Motor)
- Sensory Function: Provides sensation to the face and scalp; conducts sensory information from the skin, mucous membranes, and teeth.
- Motor Function: Controls muscles of mastication (chewing).
Abducens Nerve (CN VI):
- Function: Motor
- Function: Controls movement of the lateral rectus muscle of the eye.
Facial Nerve (CN VII):
- Function: Mixed (Sensory and Motor)
- Sensory Function: Provides taste sensation to the anterior two-thirds of the tongue.
- Motor Function: Controls facial expression muscles and stimulates salivary glands.
Vestibulocochlear Nerve (CN VIII):
- Function: Sensory
- Function: Responsible for hearing (cochlear portion) and balance and spatial orientation (vestibular portion).
Glossopharyngeal Nerve (CN IX):
- Function: Mixed (Sensory and Motor)
- Sensory Function: Provides taste sensation to the posterior one-third of the tongue and monitors blood pressure and oxygen levels in the blood.
- Motor Function: Controls swallowing muscles and stimulates parotid salivary gland.
Vagus Nerve (CN X):
- Function: Mixed (Sensory and Motor)
- Sensory Function: Monitors and regulates visceral functions of the thoracic and abdominal organs.
- Motor Function: Controls muscles of the pharynx and larynx, and regulates heart and digestive functions.
Accessory Nerve (CN XI):
- Function: Motor
- Function: Controls muscles involved in head movement (sternocleidomastoid and trapezius muscles).
Hypoglossal Nerve (CN XII):
- Function: Motor
- Function: Controls muscles of the tongue for speech and swallowing.
As mentioned above, these cranial nerves play crucial roles in controlling various functions of the head and neck, including sensory perception, motor movements, and autonomic control.
Pinched nerve symptoms and causes
Nerves follow various “routes” in the body. Some of them pass in very narrow bone “gates” or passages; some of them pass through muscles, and so on. Let’s take an obvious case like the sciatic nerve to make things easier.
The sciatic nerve – as we have discussed earlier – originates from the lumbars and sacral segments. It leaves the pelvis through a passage called “greater sciatic foramen”, to go directly under a gluteal muscle called “piriformis”. In a small percentage of the population, it passes through the piriformis. The piriformis is a short and thick muscle which can become quite tight and “chunky”, especially in runners. If this muscles becomes thick enough, it can “pinch” or “trap” or compress the sciatic nerve.
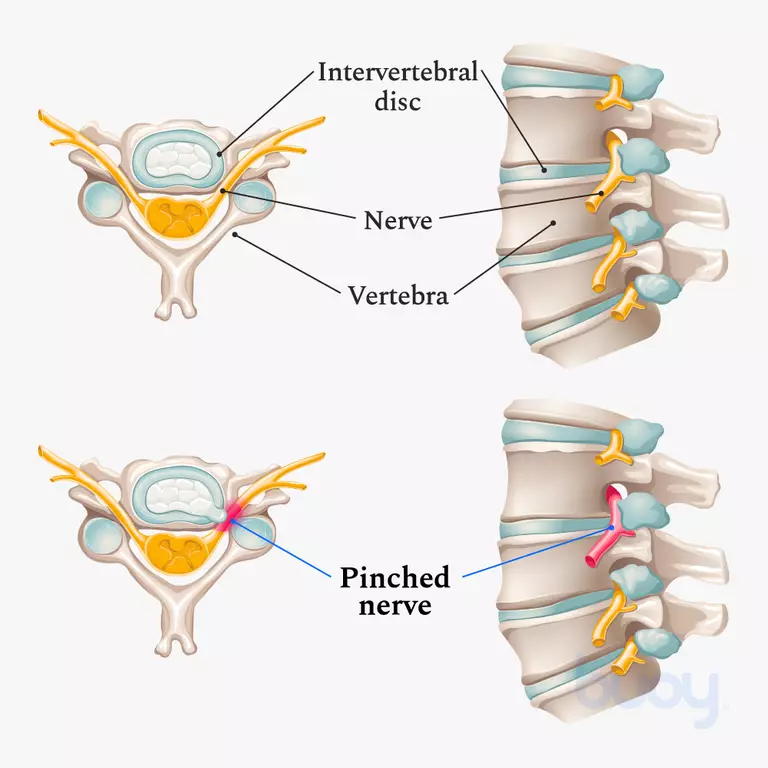
Another site of entrapment could be the spine, for example due to a build up of calcium in the intervertebral foramen. These bone spurs (or technically, osteophytes), can arise anywhere in the spine, commonly in the cervical and lumbar area. Like the example of the piriformis muscle mentioned above, they can “compress” and irritate the nerve, giving origin to a variety of unwanted symptoms.
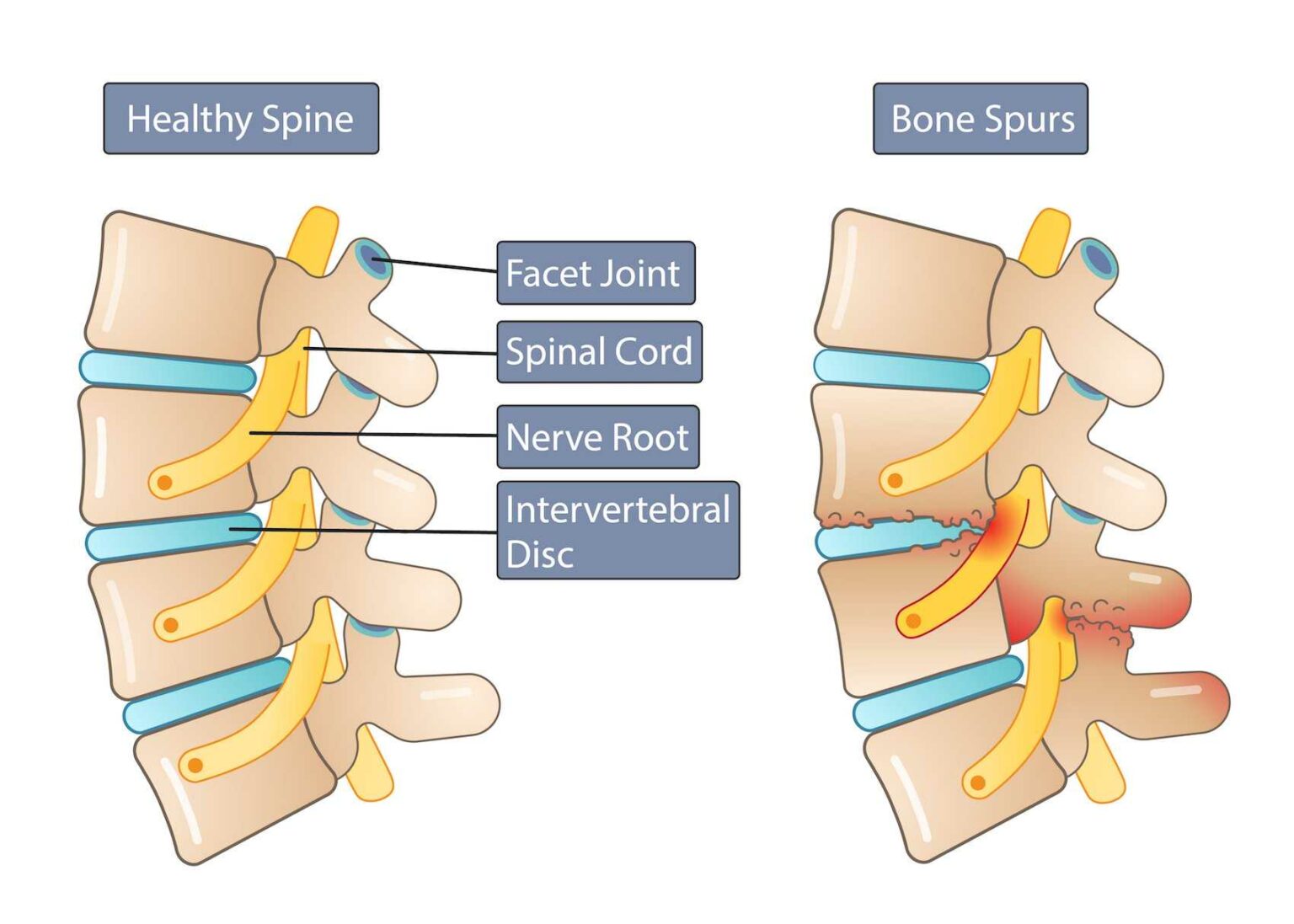
Image credit: Miami neuroscience center
Symptoms
Medical treatments for severe pinched nerve pain
When people come to see me at the clinic – and they are suffering from a nerve compression anywhere in the body – they are usually on pain killers. In the mildest cases, paracetamol and NSAIDs such as ibuprofen; in the most severe cases, medications of the calibre of Tramadol, Gabapentin, Amitriptyline. When the pain is unbearable, morphine.
Natural remedies for pinched nerve pain
There are things that objectively help to relieve the pain and will help to speed up recovery time.
Getting extra sleep and rest is a must; adapting and re-evaluating postural habits such as how to sit on the desk; ice and heat (according to the inflammatory stage); some stretches, and obviously, chiropractic.
When to seek immediate care
There are cases (luckily rare cases) where the compression could be that severe to cause very serious problems. I am talking about Cauda Equina Syndrome (CES) which is a severe compression of some lower back nerves (the cauda equina). Symptoms include radiating pain to the legs, numbness in the groin and genital area, sometimes incontinence (because those nerves provide control of the bladder aswell). As chiropractors, we are really aware of the dangers of CES and during the first consultation (at least here at Alive chiropractic) we always screen for CES when anyone presents with lower back pain. For an overview of the red flags associated with lower back pain, please visit this LINK.
Chiropractic care for pinched nerve alleviation
I could say that “pinched nerves” fall right at the centre of chiropractic care. That’s what we do on a daily basis, we open the gap through which nerves pass, and let the body do the rest. Traditionally, chiropractors do not do anything else. We have the knowledge to deal with knee injuries, ankles, wrists etc but at the core, taking pressure of the nerves is what we do. Chiropractic works generally very well for these type of problem; however the best course of action is always to get diagnosed first. The process of diagnosis is in my opinion the most important process in chiropractic care: how can we know if we can help someone, if we do not know what’s going on first? This is why diagnosis is one of the main subjects during the education years at college.
Pinched nerve recovery time and expectations
It depends. It depends from the type of problem (is it an osteophyte, a disc herniation, a muscle which is “pinching”), the severity of the problem, the chronicity (how long it has been going on for), and so on. Generally speaking – with conservative care, you can expect to improve within 2-3 weeks, but it also depends from frequency of care (how often), type of treatment etc.
Edoardo Elisei DC
Alive Chiropractic LTD
alivechiropractic.co.uk
1C Crown Gate Square
POUNDBURY
01305602314
Alive Chiropractic Poundbury
1C Crown gate square DT1 3EJ
Poundbury, Dorchester
Phone Number
01305602314
07845096314